

Can Allergies Cause Ear Pain and Blocked Ears? Causes and Treatments Explained
Written by: Dr.Muhammad Ihsan Ullah, PhD
Medically reviewed by: Dr Ali Raza Dogar ,MBBS,ENT
Last updated on May 29,2026
Yes, allergies can cause ear pain, ear pressure, fullness, muffled hearing, and a blocked ear sensation. These symptoms are often due to Eustachian tube dysfunction caused by allergies, which affects how your ear regulates pressure. While many people associate allergies with sneezing, itchy eyes, and sinus congestion, they are also a common cause of ear pressure from allergies and blocked ears during allergy season. Understanding how allergies cause muffled hearing and ear fullness is crucial for finding effective treatments and managing symptoms.

That surprises many people because allergies are usually associated with sneezing, itchy eyes, a runny nose, or sinus congestion. But the ears, nose, and throat are closely connected. When allergic inflammation affects the tissues around the Eustachian tube—the small passage that helps equalize pressure in the middle ear—your ears can start to feel clogged, tight, painful, or “underwater” (Yu, X., et al. 2024; Klimek, L., et al. 2025).
For many people, the first symptom is not severe pain. It is more often a feeling of pressure, fullness, popping, crackling, or temporary muffled hearing. In some cases, the pressure becomes uncomfortable enough to feel like a true earache. In others, fluid can build up behind the eardrum, which may make the ear feel blocked for days or even weeks if the underlying allergy flare is not controlled (Yu, X., et al. 2024; Kim, H. Y. 2025).
This is why people often ask their healthcare providers like:
- can allergies cause ear pain
- can allergies cause ear pressure
- can allergies cause blocked ears
- why do my ears feel clogged during allergies
- can seasonal allergies cause muffled hearing
- can allergies make your ears feel plugged
- can allergies cause ear fullness
All of those questions point to the same core issue: allergy-related Eustachian tube dysfunction and middle-ear pressure changes (Yu, X., et al. 2024).
If you want the direct answer in one line:
Yes, allergies can cause ear pain, pressure, fullness, and blocked ears, mainly by triggering inflammation that disrupts Eustachian tube function and sometimes contributes to fluid buildup in the middle ear (Yu, X., et al. 2024; Klimek, L., et al. 2025).
How Allergies Affect the Ears
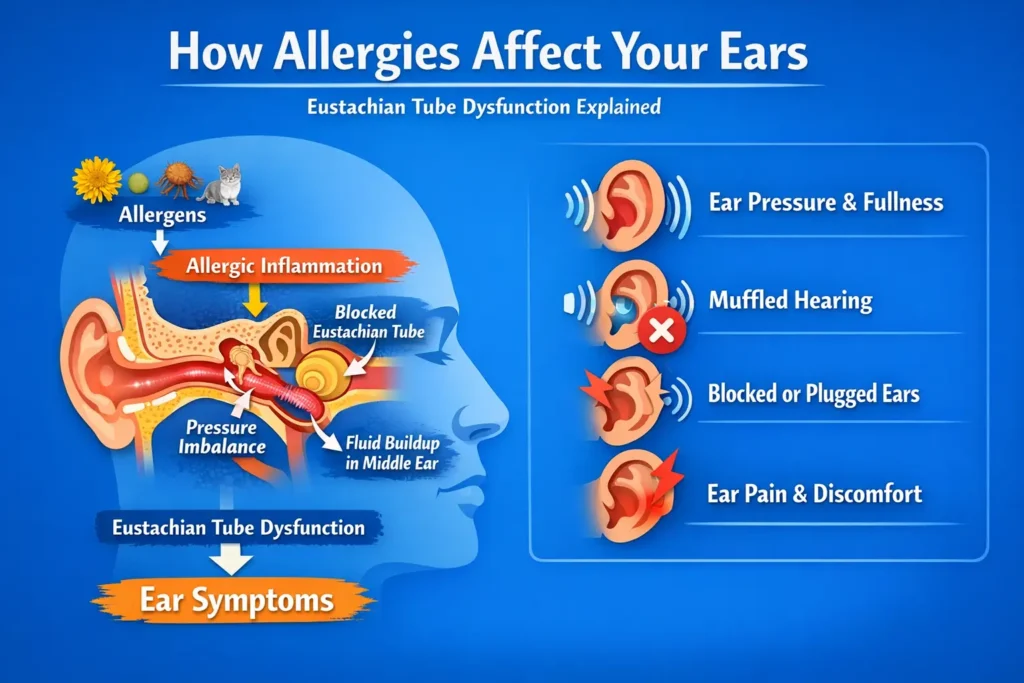
The key structure here is the Eustachian tube. This narrow channel connects the middle ear to the back of the nose and upper throat. Its main jobs are to:
- balance pressure on both sides of the eardrum
- allow normal airflow into the middle ear
- help clear secretions from the middle ear
When allergies flare up, the lining of the nose and nasopharynx becomes inflamed. That swelling can extend to the opening of the Eustachian tube. Once the tube does not open well, pressure regulation becomes abnormal, and that is when symptoms start: blocked ears, fullness, pressure, popping, muffled hearing, and sometimes pain (Yu, X., et al. 2024; Kim, H. Y. 2025).
This is why allergy-related ear symptoms often happen alongside:
- nasal congestion
- sneezing
- postnasal drip
- itchy nose or eyes
- sinus pressure
The ear symptoms are not separate from the allergy flare. They are often part of the same upper-airway inflammatory process (Bernstein, J. A., et al. 2024).
Why Allergies Can Cause Ear Pressure
Ear pressure is often the first thing people notice.
You may feel:
- one ear or both ears are “stopped up”
- your ears need to pop but will not
- your hearing feels dull
- your own voice sounds louder inside your head
This happens because the middle ear is supposed to stay ventilated. When the Eustachian tube does not open properly, pressure can become negative inside the middle ear. That changes how the eardrum moves and creates the sensation of pressure, fullness, and blockage (Yu, X., et al. 2024; Kim, H. Y. 2025).
In simple terms, your ear feels blocked not because something is physically stuffed in the ear canal, but because the pressure system behind the eardrum is not working normally (Kim, H. Y. 2025).
Can Allergies Cause a Blocked or Plugged Ear Feeling?
Yes. This is one of the most common allergy-related ear complaints.
People describe it in different ways:
- blocked ears
- plugged ears
- clogged ears
- fullness in the ear
- underwater sensation
- muffled hearing
These descriptions are usually pointing to the same mechanism: impaired middle-ear ventilation from Eustachian tube dysfunction (Yu, X., et al. 2024).
This is also why allergy-related blocked ears can come and go. On some days, the inflammation is milder and the tube opens better. On other days—especially during heavy pollen exposure, dust exposure, or worsening congestion—the blockage feeling becomes much more noticeable (Bernstein, J. A., et al. 2024).
Can Allergies Cause Ear Pain?
Yes, but the pain is often different from the pain of an acute ear infection.
Allergy-related ear pain is more often:
- dull
- pressure-like
- aching
- intermittent
- linked with fullness or popping
The discomfort usually comes from pressure imbalance, retraction of the eardrum, and irritation within the middle-ear system, rather than from a bacterial infection. If the pressure persists long enough or fluid accumulates, the discomfort can become more obvious and more bothersome (Kim, H. Y. 2025; Klimek, L., et al. 2025).
That said, severe pain should never be brushed off automatically as “just allergies.” If the pain is intense, associated with fever, drainage, or marked hearing loss, a different diagnosis such as infection may need to be considered (Klimek, L., et al. 2025).
Why Muffled Hearing Can Happen During Allergies
When pressure is abnormal or fluid collects in the middle ear, sound is transmitted less efficiently. That can lead to a temporary reduction in hearing clarity. People often describe this as:
- muffled hearing
- sounds being far away
- needing others to repeat themselves
- hearing as if under water
This type of hearing change is often conductive, meaning the problem is with sound transmission through the middle ear rather than damage to the inner ear itself. Recent review data on Eustachian tube dysfunction and hearing pathways supports this mechanism, including the effects of negative pressure and effusion on sound conduction (Kim, H. Y. 2025).
Can Allergies Lead to Fluid Behind the Eardrum?
They can.
If the Eustachian tube remains dysfunctional, fluid may build up in the middle ear. This is often called otitis media with effusion or middle-ear effusion. It does not always mean infection. Sometimes it reflects ventilation failure and inflammation rather than bacteria (Klimek, L., et al. 2025).
This is an important point because many people assume any ear pressure or fluid must mean they need antibiotics. That is not always true. In allergy-related cases, the more important step may be treating the underlying inflammation and restoring Eustachian tube function rather than automatically assuming a bacterial cause (Klimek, L., et al. 2025; Bernstein, J. A., et al. 2024).
Common Ear Symptoms Allergies Can Cause
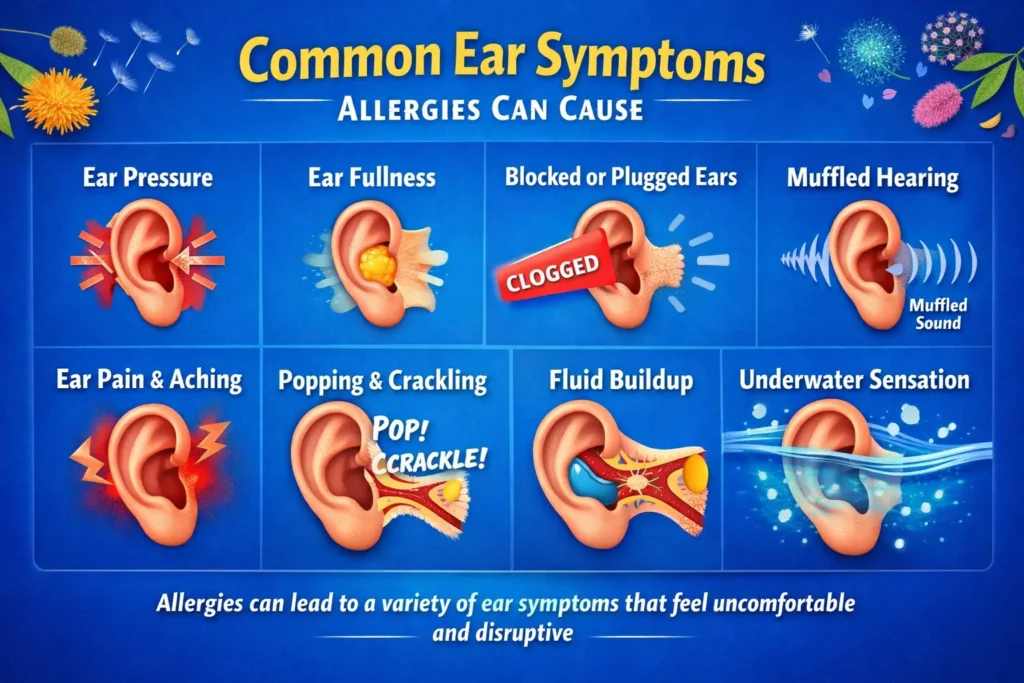
Allergies can affect the ears in several ways. The most relevant symptoms for this topic include:
- ear pressure
- ear fullness
- blocked or plugged ears
- mild to moderate ear pain
- muffled hearing
- popping or crackling
- needing to swallow repeatedly to “open” the ears
- intermittent changes that worsen during allergy flares
These symptoms are especially likely when nasal congestion is prominent, because congestion around the back of the nose can interfere with Eustachian tube opening (Yu, X., et al. 2024; Bernstein, J. A., et al. 2024).
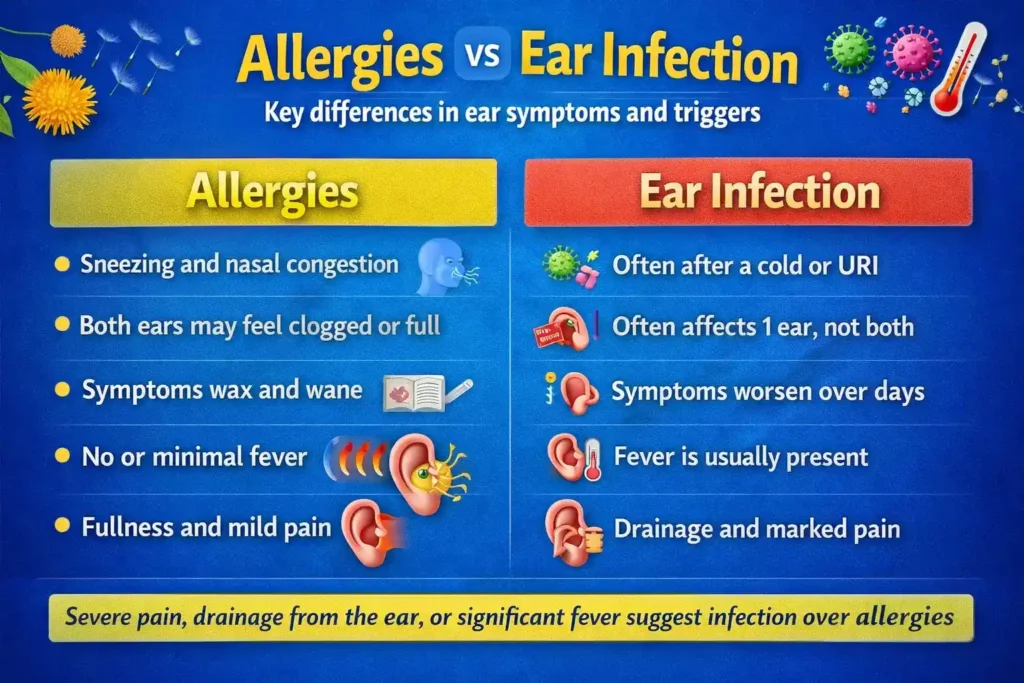
Allergies vs Ear Infection
This is one of the most important clinical distinctions.
Features that may fit allergies more closely
- symptoms come with sneezing, itchy eyes, or nasal congestion
- both ears may feel full or blocked
- symptoms wax and wane
- there is little or no fever
- the main sensation is pressure or fullness rather than severe pain
Features that may suggest ear infection or another problem
- severe or worsening ear pain
- fever
- ear drainage
- symptoms after a recent viral illness that keep worsening
- significant hearing loss
- marked tenderness or feeling very unwell
Allergies can mimic some infection symptoms, especially fullness and discomfort, but severe pain, drainage, and systemic illness deserve medical assessment (Klimek, L., et al. 2025).
Why Ear Symptoms May Feel Worse During Allergy Season
Seasonal allergic rhinitis can sharply increase inflammation in the upper airway. During high pollen seasons, many patients notice:
- more nasal obstruction
- more sinus pressure
- more postnasal drip
- more ear fullness and popping
That pattern makes physiological sense. More allergic inflammation around the nose generally means a greater chance that the Eustachian tube opening is also affected (Bernstein, J. A., et al. 2024).
Perennial allergies, such as dust mite or pet dander allergy, can do the same thing year-round. The difference is that the symptoms may feel more chronic and less obviously seasonal (Bernstein, J. A., et al. 2024).
What Usually Helps Allergy-Related Ear Pressure or Blocked Ears
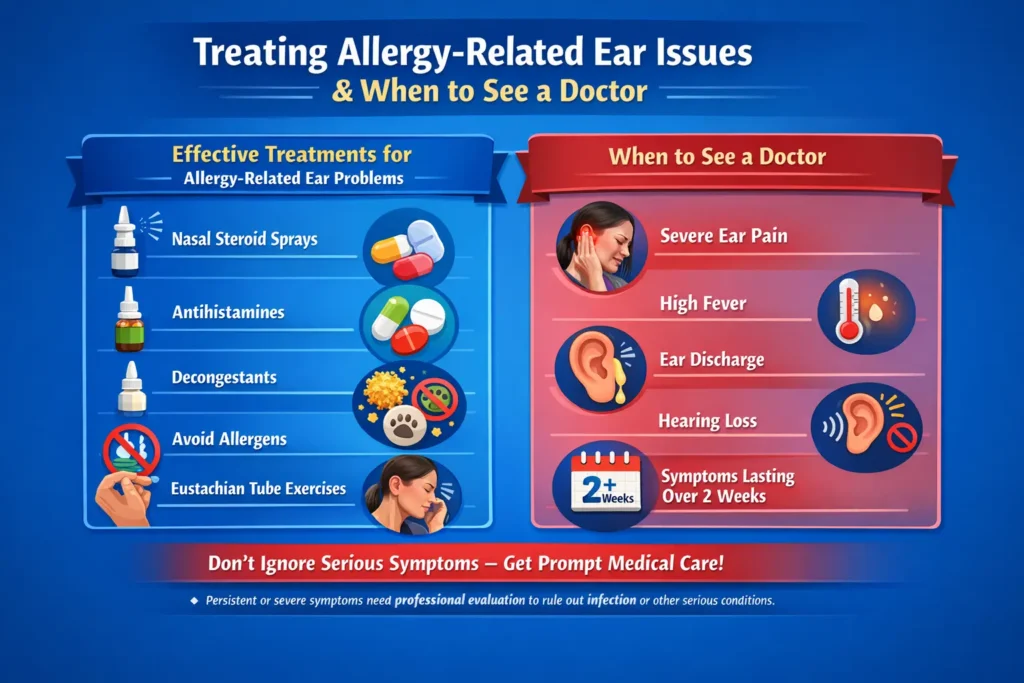
The best treatment is usually aimed at the allergy and the inflammation driving the Eustachian tube dysfunction.
1.Intranasal corticosteroid sprays
These are a mainstay for allergic rhinitis and are strongly supported in recent reviews. They help reduce inflammation in the nose and around the Eustachian tube opening, which can improve pressure regulation over time (Bernstein, J. A., et al. 2024).
Common examples include fluticasone, mometasone, budesonide, and triamcinolone. They usually work best when used correctly and consistently rather than only once in a while (Bernstein, J. A., et al. 2024).
2.Intranasal antihistamines or combination intranasal therapy
Recent evidence supports intranasal therapy as an important treatment pathway in allergic rhinitis. Systematic review data show that intranasal antihistamines and corticosteroids improve allergic rhinitis symptoms and quality of life, with differences among individual agents (Sousa-Pinto, B., et al. 2024).
3.Second-generation oral antihistamines
These can be helpful, especially when itching, sneezing, and watery symptoms are prominent. They may not directly “pop” the ears, but by reducing the overall allergic response they can help the upper-airway inflammation that contributes to ear symptoms (Bernstein, J. A., et al. 2024).
Examples commonly used in practice include loratadine, cetirizine, and fexofenadine (Bernstein, J. A., et al. 2024).
4.Allergen avoidance
If you know your trigger, reducing exposure matters. For some patients that means:
- keeping windows closed during heavy pollen days
- showering after outdoor exposure
- controlling indoor dust exposure
- using bedding protection for dust mites
- reducing pet dander exposure when relevant
Avoidance will not instantly clear blocked ears, but it can reduce the inflammatory burden that keeps symptoms going (Bernstein, J. A., et al. 2024).
Time and pressure normalization
Some allergy-related ear pressure settles as the allergy flare improves. Repeated swallowing, yawning, and gentle pressure equalization may help some people, but forceful maneuvers should be used carefully, especially if pain is significant or the diagnosis is uncertain. Persistent symptoms deserve evaluation rather than repeated self-treatment (Klimek, L., et al. 2025).
What the Latest Evidence Suggests
The most clinically useful recent evidence points in a consistent direction:
- allergy can contribute to Eustachian tube dysfunction and middle-ear symptoms (Yu, X., et al. 2024).
- allergy and immunity are important considerations in otitis media with effusion and Eustachian tube dysfunction, especially when symptoms are persistent or recurrent (Klimek, L., et al. 2025).
- modern allergic rhinitis management continues to favor anti-inflammatory intranasal treatment as a core strategy (Bernstein, J. A., et al. 2024).
- meta-analysis data show that intranasal medications are effective for improving rhinitis symptoms and quality of life (Sousa-Pinto, B., et al. 2024).
That means the question is no longer whether allergies can affect the ears at all. They can. The more practical question is whether the person’s ear symptoms fit allergy-driven Eustachian tube dysfunction alone or whether another diagnosis also needs attention (Yu, X., et al. 2024; Klimek, L., et al. 2025).
When to See a Doctor
You should not ignore ear symptoms that are severe, one-sided, or persistent.
Seek medical assessment if you have:
- severe ear pain
- fever
- drainage from the ear
- notable hearing loss
- symptoms lasting more than a couple of weeks
- recurrent episodes that keep coming back
- dizziness that is significant or worsening
- symptoms mainly in one ear and not improving
Those features can point to infection, prolonged effusion, more significant Eustachian tube dysfunction, or another ENT issue that needs direct examination (Klimek, L., et al. 2025).
Key Takeaway
If you have been wondering, “Can allergies cause ear pain, pressure, or blocked ears?” the answer is yes.
The most likely reason is not wax in the ear canal. It is usually allergy-related inflammation affecting the Eustachian tube and middle-ear pressure system. That can make your ears feel blocked, full, painful, or muffled, and in some cases it can contribute to fluid behind the eardrum (Yu, X., et al. 2024; Klimek, L., et al. 2025).
The most evidence-based approach is to address the underlying allergic inflammation, especially with appropriate rhinitis treatment, while staying alert for warning signs that suggest infection or another ear disorder (Bernstein, J. A., et al. 2024; Sousa-Pinto, B., et al. 2024).
Medical Disclaimer
This content is for informational and educational purposes only and is not intended as medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional or your physician regarding any medical concerns or symptoms. Do not ignore professional medical advice or delay seeking care based on the information provided in this article.
Frequently Asked Questions (FAQs)
1. Can allergies cause ear pain?
Yes. Allergies can trigger inflammation and pressure changes that lead to ear pain or discomfort.
2. Can allergies make your ears feel blocked or plugged?
Yes. Allergies can affect the Eustachian tube and create a blocked, clogged, or full ear sensation.
3. Can allergies cause ear pressure without an infection?
Yes. Ear pressure is commonly caused by allergy-related swelling and poor pressure equalization, even without infection.
4. Can allergies cause muffled hearing?
Yes. When pressure builds up or fluid collects in the middle ear, hearing may sound muffled or underwater.
5. When should I see a doctor for allergy-related ear symptoms?
See a doctor if you have severe pain, fever, ear drainage, major hearing loss, or symptoms that do not improve.
References
- Yu, X., Zhang, H., Zong, S., & Xiao, H. (2024). Allergy in pathogenesis of Eustachian tube dysfunction. World Allergy Organization Journal, 17(1), 100860. doi:10.1016/j.waojou.2023.100860.
- Klimek, L., Brough, H. A., Arasi, S., Toppila-Salmi, S., Bergmann, C., Jutel, M., Bousquet, J., Hox, V., Gevaert, P., Tomazic, P. V., Rondón Segovia, C., Cingi, C., Cuevas, M., Gröger, M., Huber, P., Reitsma, S., Rudenko, M., Maza-Solano, J., Gane, S., … Torres Jaén, M. J. (2025). Otitis media with effusion (OME) and Eustachian tube dysfunction: The role of allergy and immunity—An EAACI position paper. Allergy, 80(9), 2429–2441. doi:10.1111/all.16554.
- Bernstein, J. A., Bernstein, J. S., Makol, R., & Ward, S. (2024). Allergic rhinitis: A review. JAMA, 331(10), 866–877. doi:10.1001/jama.2024.0530.
- Sousa-Pinto, B., Vieira, R. J., Brozek, J., Cardoso-Fernandes, A., Lourenço-Silva, N., Ferreira-da-Silva, R., Ferreira, A., Gil-Mata, S., Bedbrook, A., Klimek, L., Fonseca, J. A., Zuberbier, T., Schünemann, H. J., & Bousquet, J. (2024). Intranasal antihistamines and corticosteroids in allergic rhinitis: A systematic review and meta-analysis. Journal of Allergy and Clinical Immunology, 154(2), 340–354. doi:10.1016/j.jaci.2024.04.016.